



Vivid Views of the Immoral COVID-19 Vaccination Gap that is Guaranteed to Prolong the Pandemic
A World Bank functionary has excelled at conveying the stark imbalance in the global response to the pandemic; can rich nations fill the deadly gap?

SUBSCRIBE to receive my twice-weekly dispatches by email - content always free so no one is left behind.
[Updated with more on nasal vaccines and other strategies that could fill the vaccination gap.]
Philip Schellekens could do just fine in his career as one of those valuable but invisible functionaries deep in the World Bank - in his case a senior economic advisor to two important groups and author of reports on demographic dynamics affecting efforts to achieve the Sustainable Development Goals.
He developed a penchant for global engagement through a decade (so far) on Twitter at @fibke. But it was in the pandemic that he hit his stride (and made my Twitter list of #Covid19Sanity Seekers).
From the earliest months of the pandemic nearly two years ago, Schellekens had been putting his demographic skills to work. In May 2020, well before vaccines emerged, Schellekens and a World Bank colleague, Diego Sourrouille, had warned in a working paper that poor countries, which then had 85 percent of world population but only 21 percent of reported deaths, were bound to suffer most in the long run. The prime reason was simple population realities - like poorer countries having 2.4 times as many citizens over age 60 as rich ones.
Their warning has been borne out, sadly.
But one year ago, propelled by the grotesque imbalance in COVID-19 vaccination levels in rich, middle-income and poor countries, Schellekens launched pandem-ic.com, a website of visualizations that are a powerful prod to the powers that be - if you and I help spread them and press for change.

from pandem-ic.com
Dozens of wonderful public-health practitioners, scholars, journalists and analysts have endured countless assaults for trying to maintain a solutions focus amid the persistent "infodemic" surrounding the pandemic. Two here on Bulletin are the physicians Jeremy Faust and James Hamblin.
For the vital global view, keeping in mind the COVID-19 pandemic can only be fully managed through global effort, I hope you'll follow Schellekens.
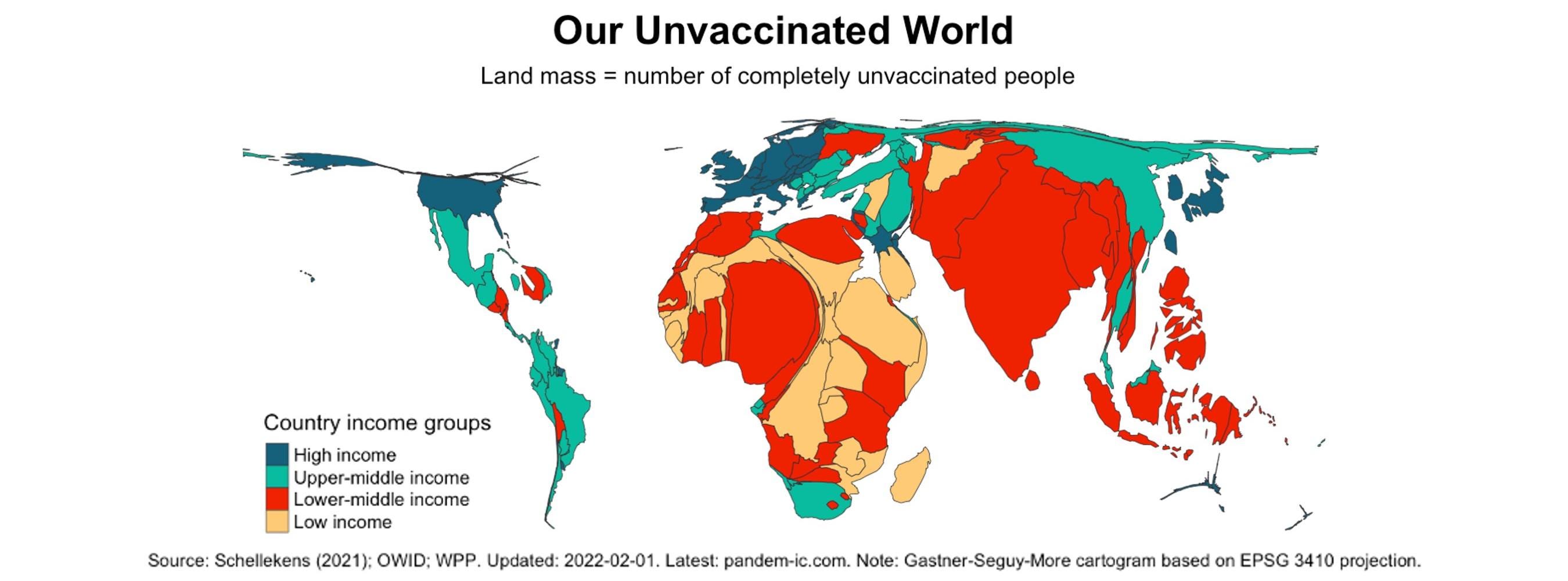
As the global vaccination effort celebrated its 10 billionth administered dose last week - an astonishing achievement - Schellekens posted a cartogram of deadly vaccination gaps. (A cartogram is a map with the familiar shapes of places distorted to represent some important variable.)

"That surely is an accomplishment," he wrote. "Within record time, 4 billion people became fully vaccinated, 1 billion among them boosted and 750 million partially vaccinated."
But, he noted, having 3 billion people still complete unvaccinated creates both an immoral death toll in places where health care is already minimal and gives the SARS-CoV-2 virus a rich biological playing field from which new variants will inevitably emerge.
Schellekens described the moral and practical reasons for vaccine gap filling this way:
"First and foremost, vaccine equity is based on a moral prerogative: to afford everyone an equal ability to protect her- or himself. Second, and only second, the enlightened self-interest argument: no one is safe until everyone is safe. We need to vaccinate the world to get the negative externalities under control."
On that second point, he's hardly alone.
From arm jab to nasal spritz
In a column just published in The Hill, a high-powered trio of pandemic experts reinforced the urgency of finally achieving global coverage as they pressed the vaccine-development and distribution community to focus more on "intranasal" vaccines that have far greater utility in world regions most in need:
"The most important factor in the emergence of variants is unvaccinated people within whom SARS-CoV-2 reproduces and evolves to even greater fitness for growth in humans. Global vaccination is the only way for us to starve the virus of the opportunity for creating additional new variants."
One author, the epidemiologist Larry Brilliant, made the case for a nose-delivered vaccine this way in an email to a batch of contacts, me included: "We won't be able to get vaccine to the 1 or 2 billion people at the 'last mile' with vaccines that require refrigeration and injection by trained health workers."
He's the chief executive officer of Pandefense Advisory, a former member of the World Health Organization Smallpox Eradication Program and chief executive of the Skoll Global Threats Fund. The other authors were Lisa Danzig, an infectious disease physician and vaccine expert with Pandefense Advisory and former epidemiological intelligence officer at the Centers for Disease Control, and Prevention, and W. Ian Lipkin, an epidemiologist who directs the Center for Infection and Immunity at Columbia University and is founding director of the Global Alliance for Preventing Pandemics.
Nasal vaccines are starting to advance, as Apoorva Mandavilli just reported for The New York Times.
This remarkably readable open-access paper from November in Drug Discovery Today makes the case, as well: "Intranasal vaccines for SARS-CoV-2: From challenges to potential in COVID-19 management." Here's the graphical abstract:

From a paper on nasal vaccine delivery by Vivek P. Chavda, Lalitkumar K. Vora, Anjali K.Pandya, and Vandana B. Patravale, Drug Discovery Today
But much time has been lost, and the vaccination gap is achingly wide, as Schellekens shows in a dynamic "vaccine donut" graph that I call the wheel of misfortune. As he's been saying, "Let's turn this donut blue." The latest data are here.
Update, 6 February: The epidemiologist Larry Brilliant sent a followup note stressing that nose-delivered vaccines are just one path to true vaccine efficacy:
"The two most important things we need from next-generation vaccines," Brilliant said, "are 1) mucosal immunity to prevent infection and 2) portability so the vaccine can be carried to the remote corners of the world, vaccinating the unvaccinated and hard to reach 1+ billion living in the 'last mile.' Yes, nasal sprays, but also oral drops (polio) and even some skin patches or freeze dried vaccines given inter dermal."
Your turn
Who are your trusted guides in this pandemic, and what builds your sense of trust in them? Please weigh in below or on Facebook. And do share this post.
Related
Before I launched this Sustain What newsletter, I ran dozens of Sustain What webcasts on the pandemic, including many on vaccination challenges. This one is most relevant, from March 12, 2021: "Can Trade Innovation Avert a Global Vaccination “Moral Failure"? I tweeted a string of key takeaways here.
A parting tweet
Schellekens is still at it of course and posted anew today:
Help build Sustain What
Any new column needs the help of existing readers. Tell friends what I'm up to by sending an email here or forwarding this introductory post.
Thanks for commenting below or on Facebook.
Subscribe here free of charge if you haven't already.
Send me feedback (including corrections!), tips, ideas here.
Find my social media accounts, books and music in a click here. And please share Sustain What with solution-focused friends and colleagues!